Vote Yes on 115 to restrict abortion after 22 weeks in Colorado

Introduction
Late abortions (after 22 weeks gestational age) are extreme by any national and international comparison. Just seven of the 50 States in the US permit abortion after 25 weeks.1 Most (38) prohibit abortion at 22 weeks or less. Internationally, only five of the 198 countries, independent states, and semi-autonomous regions with populations exceeding 1 million permit elective abortion after 24 weeks.2 Three of the five nations that permit late abortion are notorious human rights abusers: China, North Korea, and Vietnam. Colorado should not aspire to join the ranks of the few states and countries that dehumanize the developing fetus and permit the killing of these most vulnerable human beings. Colorado should also not jeopardize the health of Colorado women by allowing the unregulated out-patient practice of late abortion which is known to pose serious risks to the health and life of the woman.3
Late abortion is predicated on the notion that a woman’s right to bodily autonomy trumps the human fetus’ right to life. Both prolife and prochoice advocates would agree that a woman’s autonomy is an extremely important value; however, both sides differ on whether autonomy supersedes another human being’s fundamental right to life. These competing rights are why proponents of access to late abortion go to extreme lengths to minimize the humanity of the fetus. They refer to “terminating the pregnancy” as if the termination could occur without killing a vital, developing human being. A recent series on abortion rights by the Editorial Board of The New York Times refers to the developing human merely as a “cluster of cells” as if her brain, heart, circulatory system, appendages, hands/feet and nervous system were immaterial.4 Planned Parenthood of the Rocky Mountains characterizes the dismemberment of late second trimester fetus during a Dilation and Evacuation (D&E) abortion as removing “pregnancy tissue”.5 Orwellian language is utilized to refer to the crushed and dismembered human fetus as “products of conception” or simply “POC”. Even the preferred term “fetus” is an attempt to dehumanize the developing human. OB-GYN physicians commonly refer to the “baby” during a woman’s wanted pregnancy, but abortionists will rarely refer to the “fetus”, much less use the term “baby”, when counseling a woman on abortion.
There is little doubt that there is a bipartisan consensus that late abortions should be regulated. According to a 2018 Gallup poll, only 18% of Democrats, 13% of Independents, and 6% of Republicans believe that third trimester abortions should be legal.6 In 2020, the Marist Poll found that 70% of Americans felt that abortion should be restricted to the first 3 months of pregnancy or less.7 The Marist poll also revealed that 41% of self-identified prochoice voters were more inclined to vote for a candidate who supported abortion restrictions. The polling presumably reflects the public’s widespread recognition that late abortion kills a human being not materially different than a newborn infant and that late abortion represents a substantial medical risk to the pregnant woman.
Is the 22 week fetus a human being?
Human embryology has long established the fact that human life begins at fertilization and that human development is a seamless process that continues for years after birth. It should not be surprising that 96% of 5577 biology scientists who were recently surveyed agreed that human life begins at fertilization.8-9 No matter how hard abortion rights activists try to obfuscate, human zygotes, embryos and fetuses are biological human beings.
A primordial heart develops in the human embryo by the fifth week (post last menstrual period) and begins to pump blood by the sixth week.10 Rapid development of the brain occurs in the seventh week. By the 10th week, the embryo has distinctly human characteristics, developed the beginnings of all major organ systems, and demonstrates purposeful limb movements. During the 19th week, the mother can feel the fetal movements and by 22-weeks the fetus can respond to her mother’s touch. Fetal surgeries, in which the human fetus is operated on by specially trained fetal surgeons and anesthesiologists, have been pursued as early as the 19th- week gestation.11-12
Human fetuses have been born in the 21st-week gestation with excellent neurodevelopmental outcomes.13 Based on one national study performed on infants born at 22 weeks gestation between 2006 and 2011, 23% survived with active treatment.14 However, more recent data from the University of Iowa encompassing outcomes between 2006 and 2015, suggest a much more robust 70% survival.15 The majority had no or mild neurodevelopmental impairments.
While there is considerable debate concerning when the human fetus can experience pain, it is very likely that a 22-week-old human fetus can experience pain – likely, more intensely than an infant or adult.16 The experience of pain in humans is characterized by two neurological functions: nociception which involves the transmission of painful stimuli to the central nervous system and perception which entails the organization, identification, and interpretation of the painful sensory information. Nociception occurs early in fetal life, but perception occurs later. In a systematic multidisciplinary review published in 2005, researchers (who opposed abortion restrictions) argued that the processing of painful stimuli can only occur once the brain cortex is fully functional – not before the third trimester.17 However, the majority of contemporary fetal medicine specialists now consider the evidence that a 22-24 week fetus experiences pain compelling.16,18-22 Some believe a fetus as young as 13 weeks able to experience pain, albeit without the capacity for self-reflection.23 They cite the adequacy of nociceptive pathways, the presence of a working thalamus (which relays painful stimuli), the development of the subplate (which is an active, albeit transient, layer of the human brain cortex), documented periods of wakefulness/arousability, hormonal stress/pain responses, and fetal behavioral correlates of pain. This conclusion is reinforced by measurements of nociception-specific brain activity using near-infrared spectroscopy (NIRS), electroencephalography (EEG), and functional MRI.24-26 More sophisticated 4D ultrasound technology has also enhanced our ability to use facial expression to assess fetal pain.27-28 Because inhibitory descending pathways, which down-regulate pain perception, mature only after birth, the human fetus may be much more sensitive to pain than infants or adults.18,20-21 Clinicians have long observed that preterm infants at the lowest limit of viability have “profound, acute adverse reactions” to major painful stimuli.29 Physicians and nurses in neonatal intensive care units witness this every day and utilize multiple different pain assessment tools to help measure and mitigate the pain.19
Ultrasound using 4D technology has revealed a surprising diversity of fetal movements and added to our knowledge of the fetal central nervous system and neurobehavior.30-31 By the 11th week of gestation, the fetus demonstrates head flexion/rotation, isolated arm/leg movements, stretching, sucking, swallowing, hiccups, jaw opening and yawning.32 By the 22 weeks gestation the fetus can blink, repetitively open/close their mouth, extrude their tongue, smile, and grimace.33-34 Fetuses have been observed to cry in utero.30 These observations attest to the sophistication of the fetal brain at 22 weeks and suggest a nascent fetal emotional response.
The human fetus develops the ability to detect other sensory stimuli such as tastes and smells.35-36 Researchers have demonstrated that specific foods and flavors in the maternal diet during pregnancy can transfer to and flavor the amniotic fluid. These flavors are in turn tasted by the fetus and result in post-natal food preferences. This is how culture-specific flavor preferences are learned by the fetus and initiated early in life.
It has also long been recognized that the human fetus can respond to sound as early as 19 weeks.37-38 The human fetus specifically responds to her/his mother’s voice.39 At 25 weeks human fetuses have been observed to mimic their mother’s resuscitation of a nursery rhyme by opening and closing their mouths.40 Furthermore, a newborn human shows preference for her/his mother’s voice and for musical pieces to which she/he were previously exposed, which confirms a capacity for a fetus to learn in utero. Studies have shown that prenatally acquired acoustical memory can persist at least 6 weeks after birth.41
Late second trimester and third trimester human fetuses display a number of other advanced cortical functions. The human fetus’ sensorimotor behavior demonstrates the same characteristics later observed in the child’s behavior.40 They show curiosity or intrinsic motivation to explore their body and environment, perform repetitive actions to elicit sensations, react to sensory inputs, display intentionality, and demonstrate goal directed movements.
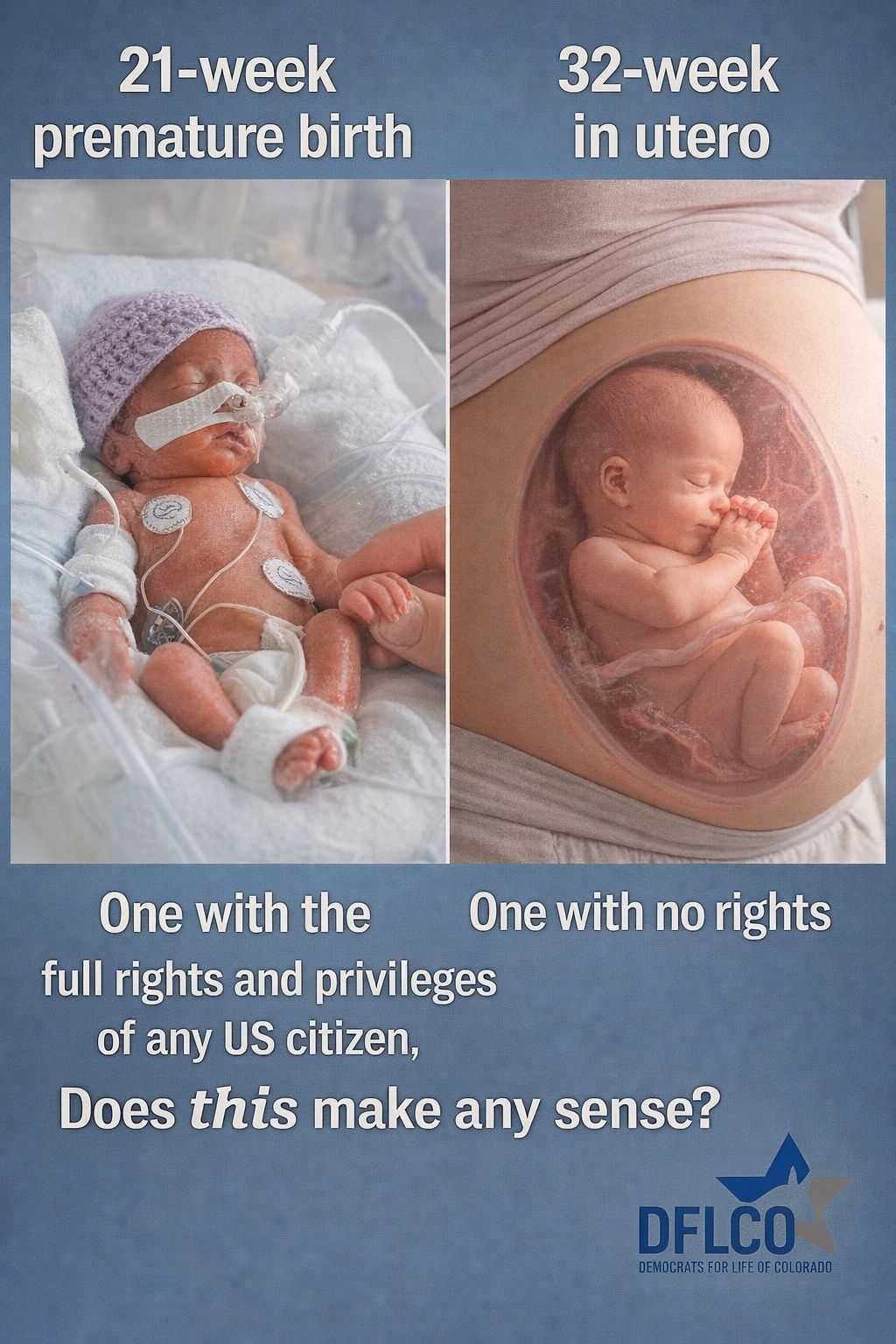
Human fetuses in utero with gestational ages of 22 weeks or greater are biologically indistinguishable from infants born at 22 weeks – they are vital human beings. They have developed all the essential organ systems, they can perceive pain, they can demonstrate sophisticated behaviors including nascent emotion, they can respond to and learn from familiar tastes and sounds, and they can undergo curative operative therapies as independent patients. The only difference is location. Location should not be the determinant of human value. A human’s inalienable right to life, proclaimed in our Constitution has not, and should not be, contingent on location.
Why do women choose late abortion, how common is the practice, and what are the alternatives?
There is very limited information available in the United States regarding who pursues very late abortions. Most studies suggest women have later abortions for similar reasons that they have early abortions with several caveats.42-44 Age and educational level were not associated with abortions after 16 weeks in one Guttmacher sponsored study.42 Black women were twice as likely to have late abortions. Another study which was based on the baseline Turnaway data concluded that “reasons for seeking abortion are not different whether women sought abortion early or late in pregnancy.”43 They did not find a statistically significant difference between early and late second trimester abortions based on finances, parity, timing of pregnancy, degree of interference with future opportunities, emotional/mental preparedness, health related reasons, prospects for the baby, level of independence/maturity, influences from family/friends or the inability to contemplate adoption. A second study based on the Turnaway data suggested statistically significant differences in the age of the woman (younger patients, later abortions OR 2.7) and time that pregnancy was recognized (before 8 weeks, earlier abortions OR 0.1).44 They also found that women who had late abortions faced more logistical delays (finding a provider, raising funds, and travel costs). Both Turnaway studies excluded abortions for fetal anomalies or life endangerment.
Many people are under the impression that most late abortions are necessitated by terrible fetal anomalies or life endangering conditions. Ron Fitzsimmons, the executive director of the National Coalition of Abortion providers, famously admitted that he lied to Congress and the public when he stated that late abortions are rare and performed primarily to save the lives of women and to prevent them the burden of bearing severely deformed babies.45-46 He stated that late abortion is performed much more commonly than acknowledged and generally on healthy women bearing healthy fetuses. He feared the truth would hurt the cause of abortion rights. This sentiment is echoed by Frances Kissling, president of the Center for Health, Ethics and Social Polity who admitted that “our talking point is, most of these procedures are on women who discover abnormalities late in the pregnancy” even though “we don’t know if that is true”.47 Late abortionists have admitted doing thousands of late abortion procedures annually and only a “minuscule amount” on abnormal fetuses.45 Hillary Clinton famously repeated the false spin that late abortions “are because of medical necessity” during a debate with candidate Donald Trump. This assertion was widely debunked by fact checkers.48 Diana Foster, Professor at the University of California San Francisco’s Bixby Center for Global Reproductive Health stated that “there aren’t good data on how often later abortions are for medical reasons”. Her opinion, based on the limited research and discussions with fellow researchers in the field, was that abortion for fetal anomalies “make up a small minority of later abortions”.48 There are other sources including investigations, blog posts, interviews and documentaries that suggest it is not hard to schedule a late abortion or uncommon to abort an entirely normal fetus after 24 weeks gestation.49-53 One of the few mandatory state databases that confidentially tracks late abortions in Arizona, reported that 80% of abortions after 21 weeks were performed on normal fetuses in 2018.54
There is no mandatory reporting for number of abortions, indications for abortions or complications from abortions in the United States. Consequently, it is difficult to independently assess the practices of late term abortionists and the patients they serve. It is also uncommon for an independent expert to review late abortionists’ practices. In a rare move that resulted in significant controversy/litigation, Kansas Attorney General Phil Kline had Dr. Paul McHugh, University Distinguished Service Professor of Psychiatry at Johns Hopkins School of Medicine, review redacted records of prominent third-trimester abortionist, George Tiller.55 Dr. McHugh reported that he found instances where abortions were obtained for “trivial reasons” (like a desire to play sports) and for psychiatric reasons (such as adjustment disorder, anxiety, and depression) that could have been more appropriately remedied without resorting to late abortion. He indicated that from his review of the records “anybody could have gotten an (third trimester) abortion if they wanted one”.
In Colorado, the Boulder Abortion Clinic advertises elective abortions, (for any reason) to 26 weeks and then to 36 weeks for “medically indicated terminations”.56 Few Colorado abortionists publicly admit performing late/third trimester abortions and Dr. Warren Hern from the Boulder Abortion Clinic is the exception. In a number of newspaper and magazine stories, the impression is given that he only performs late abortions for fatal fetal anomalies and life-endangering conditions of the mother.57-58 However, anecdotal reports and a scientific publication suggests that the Boulder Abortion Clinic is willing to consider later abortions for normal human fetuses.49, 52, 56, 59 Dr. Hern has admitted that 70% of his abortion practice is for normal human fetuses.59 In those 30% of abortions performed for fetal anomaly, he reports that Down Syndrome is his most common indication (24%). Potentially treatable structural anomalies are included in his series (such as spina bifida, aortic stenosis, abdominal wall abnormalities, urinary obstruction, extra digits, fused digits, deformed hands or feet, scoliosis, and cleft lip/palate).59
To obtain Colorado-specific abortion data is extremely difficult. The Colorado Department of Health (CDPHE) collects an (admittedly) incomplete survey of abortion providers (since it is anonymous, not mandated, and there is no enforcement mechanism). In their 2018 Report of Induced Terminations of Pregnancy, 323 abortions were performed after 21 weeks gestation in Colorado (which represents 3.6% of the total abortions performed).60 The corresponding figure for 2019 was 169 or 1.9%.61 The Guttmacher Institute pegs the abortion rate in Colorado approximately 40% higher (based on 2017 data)62 Assuming the CDPHE underestimation persists and is uniformly distributed amongst all gestational ages, this would translate into approximately 452 abortions after 21 weeks in 2018 and 237 in 2019.
There is reason to believe that late abortions are significantly under-reported In Colorado. The precipitous drop in late abortion in 2019 is not credible. Abortions dropped from 277 between 22-24 weeks gestation in 2018 to 123 in 2019.60-61 There is no plausible explanation for this drop other than a decrease in clinic(s) reporting late abortions. The notion of under-reporting is further reinforced by the observation that the Boulder Abortion Clinic can’t be reporting their figures. Dr. Hern’s own published research suggests that he was performing approximately 250 abortions per year with 70% after 22 weeks, and 40% after 26 weeks.59 The 2018 and 2019 CDPHE reports only indicate 12 and 13 abortions were performed after 25 weeks – instead of the estimated 100 abortions performed by Dr. Hern after 26 weeks alone.
How often is it medically necessary to abort a human fetus to preserve the life or health of the mother? Dr. Diane Foster from the University of California San Francisco states that the number is very hard to characterize.48 Although there is almost no literature on the subject, one Maternal-Fetal Medicine expert concludes that this is an exceedingly rare event, perhaps encompassing as few as 4 extremely uncommon conditions: pulmonary hypertension (primary or Eisenmenger’s syndrome), Marfan’s syndrome with aortic root involvement, complicated coarctation of the aorta, and peripartum cardiomyopathy with residual dysfunction.63 These would all likely be adjudicated long before 22 weeks gestation. Dr. Hern has said that he is unaware of a situation where abortion was necessary (as opposed to delivery) to save the life of a mother in the third trimester.64 When a mother has a true medical emergency after 22 weeks gestation, abortion is never the safest approach. Emergent delivery of the baby via cesarean section is considered the medically appropriate option. To pursue a multi-day abortion procedure would be widely perceived to be medical malpractice.
Some women may feel the need to abort their fetus if they discover chromosomal or structural abnormalities. Prenatal screening tests can confirm fetal abnormalities by 18-20 weeks using currently recommended national screening guidelines – first trimester screen or quadruple marker screen, or integrated stepwise sequential/contingent screening, or cell free DNA screening and mid-trimester ultrasound.65 These women who choose to abort these fetuses should not be impeded by a prohibition on abortion after 22 weeks gestation. Similarly, women who have fetuses conceived in rape and choose abortion need not be affected by late abortion restrictions.
There is no question that woman contemplating late abortion make heart-wrenching decisions. They often feel that abortion is their only choice because of lack of support from family/friends. They may be unaware of life-affirming alternatives. Women need to know that in Colorado there are many private and governmental organizations that can provide medical, financial, housing, educational, employment, adoption, emotional and spiritual support to them and their families. They should also be made aware of the many compassionate services that Perinatal hospice offers.
Perinatal loss is one of the most devastating events a family will ever experience. Tragically, many families are unaware that perinatal hospice offers a compassionate, loving, and life-affirming alternative to late abortion for fetuses with life-limiting genetic or congenital abnormalities. Perinatal hospice can improve the mother’s and family’s experience when confronted with a fatal fetal diagnosis.65-67 Perinatal hospice involves a multidisciplinary team that includes obstetricians, perinatologists, labor & delivery nurses, neonatologists, clergy, social workers, midwives and hospice professionals. Together they accompany the family through the pregnancy and birth allowing them to fully embrace and celebrate the abbreviated life of their baby. The baby receives palliative symptom management to ensure a natural and comfortable passing. The family is afforded precious time to hold, feed, bathe, and love their baby. Perinatal hospice provides ongoing bereavement services for a year or more. None of these services are typically provided with a late abortion – families are left on their own to navigate the emotionally wrenching reality of their babies illness and death – in which they were complicit.
Late abortions are performed for the same reasons that early abortions are performed. There may be more abortions for fetal anomalies late in pregnancy, but this is still likely a small proportion overall. Late abortions occur commonly in Colorado, but figures are inaccurate and lack some demographic and medical detail. Late abortions to preserve the life of the mother are a very rarely, if ever, indicated. Perinatal hospice offers a compassionate, life-affirming alternative to late abortion for families struggling with a fatal fetal diagnosis. Late abortion restrictions need not affect the choices for women with chromosomally or structurally abnormal fetuses and those suffering from rape.
How are late abortions performed and are they “humane”?
There are many different abortion techniques and remarkable procedure variability among physicians performing late second trimester and third trimester abortions. This reflects the lack of consensus in the abortion community.
Generally, beginning at 16 weeks gestation, Dilation and Evacuation (D&E) replaces sharp curettage and suction curettage as the surgical abortion procedure of choice.69 During D&E, cervical dilation is achieved over one or more days by osmotic dilators (+/- adjuvant misoprostol) to facilitate the subsequent mechanical destruction and dismemberment of the fetus. Parts of the human fetus grasped/torn from her/his torso are then easily removed through the dilated cervix. A large-bore vacuum curette is used to remove the placenta and remaining tissue. Administration of a pre-procedure feticide such as intraamniotic/intra-fetal digoxin, intracardiac potassium chloride or transection of the umbilical cord sometimes proceeds the D&E.
Dilation and Extraction (D&X) or Intact D&E is similar to the D&E procedure except that a suction cannula is utilized to evacuate the brain after delivery of the fetal human body/legs through the dilated cervix.69 The ensuing collapse of the head facilitates its passage through the cervical canal. In the popular vernacular this procedure is sometimes referred to as “Partial-Birth Abortion”. In order to comply with the Partial-Birth Abortion Ban Act of 2003, fetal demise must be ensured prior to the procedure. This is accomplished using a pre-procedure feticide or by transection of the umbilical cord.
During an Induction Abortion, labor is induced using mechanical means and/or by chemical means after several days of osmotic dilators.69 The human fetus is usually delivered intact. To remain within the framework of the law, fetal demise is achieved prior to delivery using a feticide. This is the method used in third trimester abortions.
Abortion proponents make the claim that fetal death during abortion is more compassionate and painless than natural fetal/infant death in instances where the fetus has a terminal diagnosis. However, there are no published studies comparing the pain/suffering induced during abortion vs. natural fetal/infant death. During D&E, only 30-50% of human fetuses are routinely killed prior to the dismemberment procedure in second trimester abortions.70-71 It is hard to imagine that dismemberment would be less painful than natural death in conjunction with advanced perinatal hospice/palliative care services.
Even for those human fetuses who are killed before they are dismembered or delivered in second and third trimester abortions, there may be substantial suffering. A recent post-mortem MRI study of fetuses who have been administered a feticide indicate secondary pneumothorax – collapsed lung (23%), hemothorax – hemorrhage in lung (42%), pneumopericardium – air around the heart (31%), and hemopericardium – hemorrhage around the heart (35%).72 These fetuses also had higher intraabdominal injuries. This suggests that just the process of injecting the feticide may inflict substantial pain. Furthermore, a highly concentrated potassium infusion can cause intense intravascular burning in normal patients.73 Even though an intracardiac infusion of potassium can kill a fetus within 2 minutes, It’s impossible to ascertain whether the human fetus experiences intense pain prior to its demise.74 Intraamniotic or intra-fetal digoxin is the more commonly used poison to achieve fetal demise.75 A digoxin overdose in older humans causes intense nausea, vomiting, abdominal pain, visual disturbances and delirium.76-78 Digoxin kills by causing severe bradycardia (slow heart rate) culminating in asystole (heart stopping), but it does not kill quickly. It can take up to 4 hours for intra-fetal and up to 24 hours for intraamniotic digoxin to achieve asystole.79-80 Women are routinely told to anticipate “kicks” for hours after the feticide is administered.81 The visual, gastrointestinal, neurological and cardiac manifestations of digoxin toxicity could arguably represent fetal human cruelty. Indeed, if this same methodology was utilized in a death penalty case, it would be considered “cruel and unusual punishment”.
In more candid moments, even abortion advocates sometimes characterize late abortion procedures on human fetuses as “morally abhorrent”.82 It is a form of intimate human violence which is unparalleled in medicine. The only reason that it persists is that the violence is hidden within the confines of the uterus. When the mother (and the broader public) are shielded from the reality of the carnage that is being inflicted on the human fetus, it is easier to rationalize its utility. Since there are no studies on the pain associated with late fetal abortion, to regard this as a painless, humane procedure is either wishful thinking or horribly misguided.
What is the risk to the woman undergoing a late abortion?
Late abortion is associated with significant morbidity and mortality. The precise magnitude of the risk associated with abortion can’t be reliably gleaned from the CDC or state databases because reporting abortion numbers and related complications is not consistently state mandated and never federally mandated. Furthermore, abortion procedures in the US are not linked to other sources of health data such as birth or death certificates making meaningful estimates of mortality rates nearly impossible. Since the system is voluntary and physicians are reluctant to disclose serious complications (including death), under-reporting is also a major problem.83 There have been multiple instances documented where abortion related morbidity and mortality were not captured by the official state/federal databases. Since Colorado does not have require any oversight of abortion clinics (other than low-bar licensing requirements for their nursing/physician employees), there is substantial risk that maiming and death of affected women may go unreported. The Gosnell grand jury report in Pennsylvania should serve as a sober reminder that assuming major injuries and deaths from abortion are reported to and acted upon by civil authorities or medical boards is extremely naïve.84
Even using the admittedly inadequate medical claims/surveillance data, late abortion poses a substantial risk compared to early abortion in both relative and absolute terms. Using California Medicaid billing data, Emergency Department visits and complications were 2.5 times more likely following a second trimester abortion compared to a first trimester abortion.85 Data from the national Abortion Surveillance System indicate that while the overall risk of death from abortion was 0.7/100000 induced abortions, the risk of death increased exponentially (by 38%) for each additional week of gestation.86 CDC researchers found that gestational age was the strongest predictor of abortion-related-mortality.3 In absolute terms, the risk goes from 0.1 deaths/100000 for surgical abortions < 9 weeks to 8.9 deaths/100000 at > 20 weeks.86-87 To put this in perspective, the American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF) compiled a 5 1/2 year database of over 1 million out-patient surgeries performed in ambulatory surgery centers.88 The death rate was 2/100000 for patients that were, on average, significantly older than patients undergoing late abortion. This is only 22% of the mortality rate seen in late abortion. The Canadian counterpart, the Canadian Association for Accreditation of Ambulatory Surgical Centers (CAAASF), conducted a survey that pointed to a death rate of approximately 1/100000 which represents only 11% of the risk of late abortion.89 The risk must be viewed in the context of strict oversight of ambulatory surgical centers in Colorado and the absence of oversight or regulations pertaining to abortion facilities in Colorado.90 Media Trackers reported that “while standard healthcare and out-patient surgical clinics in the state fall under the authority of the Health Facilities division of the Colorado Department of Health and Environment for regular licensing and regulation, Planned Parenthood (and other abortion providers) are not held to the same standard”. Not only does late abortion represent a significant mortality risk to women but the lack of health/safety oversight potentially compounds that risk.
Mortality studies that are based on countries with linked birth, pregnancy, abortion and death registries give an even more stark view of the risk from abortion. In Denmark, the 180-day mortality associated with late abortion (>12 weeks) was 55/100000.91 This is far worse than US surveillance data would suggest and places it in a league with neurosurgery (lumbar discectomy 60/100000), and abdominal surgery (laparoscopic appendectomy, inguinal herniorrhaphy 20/100000, laparoscopic cholecystectomy 200/100000).92-95 While this study is not adjusted for socioeconomic factors, marital status or psychological history, they suggest that mortality risk for women undergoing late abortion might be substantially underestimated in the US.
Some have tried to claim that a legal induced abortion is much safer than childbirth.96 However, others have pointed out that these studies are inherently biased and plagued with differences in ascertainment of deaths, duration of susceptibility to mortality, lack of accounting for gestational age and inappropriate comparators.83 The relative risk of pregnancy associated death between delivery and abortion may be better assessed by looking at countries with linked birth/medical/death databases. A systematic review and meta-analysis suggested that based on 11 studies from three such countries, termination of pregnancy is a marker for reduced life expectancy.97 They found that within a year of their pregnancy outcomes, women experiencing pregnancy loss (from either abortion or natural loss) were twice as likely to die compared to women giving birth. In Denmark, this adverse mortality rate persisted for 10 years.91 While there could be confounding variables complicating this analysis, the notion that abortion leads to better health outcomes is unlikely (and certainly speculative without more rigorous research).
The morbidity associated with abortion also increases with gestational age. A large retrospective study from the University of California San Francisco suggested that the complication rate for second trimester abortions was 9.8% (including cervical laceration, hemorrhage, uterine atony, anesthesia complications, uterine perforation, disseminated intravascular coagulation, and retained products of conception). Major life-threatening complications (complications requiring hospitalization, transfusion, or further surgical intervention) occurred in 1.7% of patients.98 Any of these complications increased with each additional week of gestation beyond 20 weeks. Another study observed that for each one-week increase in gestational age, there was a 7.1% increase in estimated blood loss.99 Unfortunately, there are no published studies specifically addressing the likely extremely high morbidity/mortality associated with third trimester abortions.
Long-Term health effects of abortion are controversial.3 Retrospective studies suggested a correlation of abortion with breast cancer. Better, case control studies suggested no correlation. There appears to be an association of abortion with postpartum hemorrhage in later pregnancies, but the mechanism is undefined. Late abortions may result in an increased risk for premature birth in subsequent pregnancies (aOR= 1.13, 99% CI 0.91-1.4). This trend becomes statistically significant for women who have had multiple abortions.3 Researchers have found a dose-response relationship between the number of prior abortions and the risk for extreme premature birth. The correlation between late abortion and/or multiple abortions with extremely premature birth and very low birth weight was more recently corroborated by a large Finnish national registry study.100 Since black women have, on average, more late abortions and more multiple abortions, one might speculate that the scourge of increased infant mortality (tied largely to premature birth and low birth weight infants) in the black community could be partially caused by abortion.
The adverse effects of abortion on mental health is particularly controversial. Recent reviews cited by abortion proponents rely heavily on the methodologically flawed Turnaway study to conclude that abortion is not associated with new mental health disorders.3 Better studies from Denmark utilizing national health registries suggest that abortion is a powerful marker for, rather than a cause of, affective disorders and suicide attempts.101-102 Other recent studies from America, China, and Korea suggest adverse mental health outcomes related to abortion.103-106
A balanced synthesis of the literature suggests several consensus opinions regarding the nexus between abortion and mental health:
“1) abortion is consistently associated with elevated rates of mental illness compared to women without a history of abortion,
2) the abortion experience directly contributes to mental health problems for at least some women,
3) there are risk factors, such as pre-existing mental illness, that identify women at greatest risk of mental health problems after an abortion.”107
The risk of affective disorder and suicide ideation may be even more pronounced after the abortion of a wanted pregnancy – such as for fetal anomaly or maternal indications.108 Adverse mental health associations or effects may be tied with increased mortality in women having induced abortion.91, 97, 109
Conclusions:
Late abortion is extreme by any measure and should be prohibited. Passing Proposition 115(formerly Initiative 120) is not only medically/morally correct, it is consistent with the views of a majority of Coloradans. Very few countries in the world permit abortion after 20 weeks. Most Americans, regardless of their political affiliation, feel that abortion should be illegal late in pregnancy. A 22-week fetus in biologically indistinguishable from a baby born at 22 weeks. There is scientific evidence that a 22-week human fetus demonstrates all the fundamental characteristics of more developed humans, including the ability to perceive pain and perform sophisticated behaviors. The reasons women choose late abortion are similar to the reasons that women choose early abortion. Most late abortions are performed on normal human fetuses. For those tragic situations where a human fetus has a life-limiting prognosis because of a genetic or congenital fetal abnormality, perinatal hospice offers a compassionate, life-affirming alternative to late abortion. Late abortions are violent procedures that commonly involve the crushing and dismemberment of the human fetus. Late abortions pose a substantial morbidity and mortality risk to the pregnant woman, which is further exacerbated by the lack of regulatory oversight. Long term sequelae of abortion include the risk for future premature birth and adverse future pregnancy outcomes. There may be an increased risk of early mortality in women who have abortion compared to women who deliver babies. This may be related to antecedent poor mental health in women who choose abortion and possibly adverse long-term mental health outcomes from abortion.
Thomas J. Perille MD
Head, Medical Advisory Team, Coalition for Women and Children
Democrats for Life of Colorado
Revised June 2020
References:
-
State Policies on Later Abortions. (2019, January 1). Retrieved from https://www.guttmacher.org/state-policy/explore/state-policies-later-abortions. January 10, 2019
-
Lee, M. Y. H. (2017, October 9). Is the United States one of seven countries that ‘allow elective abortions after 20 weeks of pregnancy?’. The Washington Post.
-
Committee on Reproductive Health Services. The Safety and Quality of Abortion Care in the United States. Washington DC: The National Academy Press, 2018.
-
The Editorial Board of the New York Times. (2018, December 28). A Woman’s Rights. The New York Times. Retrieved from https://www.nytimes.com/interactive/2018/12/28/opinion/abortion-murder-charge.html January 10, 2019.
-
Planned Parenthood. “What happens during an in-clinic abortion”. Retrieved from https://www.plannedparenthood.org/learn/abortion/in-clinic-abortion-procedures/what-happens-during-an-in-clinic-abortion January 4, 2020.
-
Trimesters Still Key to Abortion Views. (2018, June 13). Retrieved from https://news.gallup.com/poll/235469/trimesters-key-abortion-views.aspx. January 04, 2020.
-
Americans’ Opinions on Abortion. (2020, January). Retrieved from http://www.kofc.org/en/news/polls.html#/ June 17, 2020
-
Jacobs, S (2019) I asked thousands of biologists when life begins. The answer wasn’t popular. Quillette. Retrieved January 8, 2020 at https://quillette.com/2019/10/16/i-asked-thousands-of-biologists-when-life-begins-the-answer-wasnt-popular/?fbclid=IwAR0selWLvSvGon-YRh2SVHr62dWQkGZmNNSg-vkDYLJM2v61QHI17QlSJN0.
-
Jacobs, SA. (June 2019). Balancing Abortion Rights and Fetal Rights: A Mixed Methods Mediation of the US Abortion Debate. (Doctoral Thesis, University of Chicago, USA). Retrieved January 8, 2010 at https://knowledge.uchicago.edu/record/1883.
-
Moore, KL, Persaud, TVN, and M Torchia. The Developing Human: Clinically Oriented Embryology. 2013. Elsevier Saunders. Print.
-
Moldenhauer JS and Adzick NS. Fetal Surgery for myelomeningocele: After the Management of Myelomeningocele Study (MOMS). Seminars in Fetal & Neonatal Medicine 2017; 22: 360-366.
-
Graves CE, Harrison MR, and Padilla BE. Minimally Invasive Fetal Surgery. Clin Perinatol 2017; 44: 729-751.
-
Ahmad KA, Frey CS, Fierro MA, Kenton AB, and Placencia FX. Two-Year Neurodevelopmental Outcome of an Infant Born at 21 Weeks’ 4 Days’ Gestation. Pediatrics 2017; 140(6): e20170103.
-
Rysavy MA, et. al. Between Hospital Variation in Treatment and Outcomes in Extremely Preterm Infants. NEJM 2015; 372: 1801-1811.
-
Watkins PL, et.al., Outcomes at 18-22 Months of Corrected Age for Infants Born at 22 to 25 weeks of Gestation in a Center Practicing Active Management. J Pediatr; October 9, 2019. pii: S0022-3476(19)31086-8. doi: 10.1016/j.jpeds.2019.08.028.
-
Bellieni CV et. al., New insights into fetal pain. Semin Fetal Neonatal Med. 2019 Aug;24(4):101001. doi: 10.1016/j.siny.2019.04.001. Epub 2019 Apr 6.
-
Lee SJ, et.al. Fetal Pain: A Systematic Multidisciplinary Review of the Evidence. JAMA 2005; 294(8): 947-954.
-
Sekulic S, et.al. Appearance of fetal pain could be associated with maturation of the mesodiencephalic structures. Journal of Pain Research 2016; 9: 1031-1038.
-
Boyle EM. Measuring and managing pain in the fetus and neonate – A new era and new challenges. Semin Fetal Neonatal Med 2019 Aug;24(4):101018. doi: 10.1016/j.siny.2019.101018. Epub 2019 Jul 3
-
Maxwell LG et. al., Assessment of Pain in the Newborn: An Update. Clin Perinatol. 2019 Dec;46(4):693-707. doi: 10.1016/j.clp.2019.08.005. Epub 2019 Aug 19
-
Ranger M and Grunau RE, Early repetitive pain in preterm infants in relation to the developing brain. Pain Manag 2014; 4(1): 57-67.
-
Vinall J and Grunau RE, Impact of repeated procedural pain-related stress in infants born very preterm. Pediatr Res. 2014: 75(5): 584-587.
-
Derbyshire SWG and Bockmann JC. Reconsidering fetal pain. J Med Ethics 2020; 46:3-6.
-
Field T, Preterm newborn pain research review. Infant Behavior and Development 2017; 49: 141-150.
-
Roue JM et.al., Multi-modal pain assessment: are near-infrared spectroscopy, skin conductance, salivary cortisol, physiologic parameters, and Neonatal Facial Coding System interrelated during venipuncture in healthy term neonates? Journal of Pain Research 2018; 11: 2257-2267.
-
Relland LM, et.al., Behavioral and Physiological Signs for Pain Assessment in Preterm and Term Neonates During a Nociception-specific Response: A Systematic Review. Pediatr Neurology 2019; 20: 13-23.
-
Reissland N, Francis B, Mason, J. Can Healthy Fetuses show Facial Expressions of “Pain” or “Distress”. PLoS ONE 2013; 8(6): e65530. Doi:10/1371/journal.pone.0065530.
-
Bernardes S, et.al. On the feasibility of accessing acute pain-related facial expressions in the human fetus and its potential implications: a case report. Pain Reports 2018; 3: e673
-
McPherson C, Inder T. Perinatal and neonatal use of sedation and analgesia. Seminars in Fetal and Neonatal Medicine 2017; 22: 314-320.
-
Neto RM and Porovic S. Clinical study of fetal neurobehavior by the KANET test. J. Perinatal. Med 2018; 46(6): 631-639.
-
Kurjak A et.al., Is four-dimensional ultrasound Entering a new field of fetal psychiatry? Psychiatria Danubina 2019; 31(2): 133-140.
-
Kurjak A et.al., Fetal behavior assessed in all three trimesters of normal pregnancy by four-dimensional ultrasonography 2005; 46(5): 772-780.
-
Sato M, et.al., 4D ultrasound study of fetal facial expressions at 20-24 weeks. International Journal of Gynecology and Obstetrics 2014; 126: 275-279.
-
Lebit FD and Vladareanu R, The role of 4D ultrasound in the assessment of fetal behavior. Medica 2011; 6(2): 120-127
-
Mennella JA, Jagnow CP and Beauchamp GK, Prenatal and Postnatal Flavor Learning by Huan Infants. Pediatrics 2001; 107(6): E88
-
Spahn JM et.al., Influence of maternal diet on flavor tranfer to amniotic fluid and breast milk and children’s responses: as systematic review. Am J Clin Nutr 2019; 109(Suppl): 1003S-1026S.
-
Hepper PG, Shahidullah BS. Development of Hearing. Archives of Disease in Childhood 1994; 71: F81-F87.
-
Johnson Chacko L et.al., Growth and cellular patterning during fetal human inner ear development studied by a correlative imaging approach. BMC Developmental Biology 2019; 11: 1-14.
-
Gerhardt KJ, Abrams RM. Fetal exposures to sound and vibroacoustic stimulation. J Perinatol 2000; 20 (8 Pt2): S21-30.
-
Fagard J, et.al. Fetal Origin of Sensorimotor Behavior. Frontiers in Neruorobotics 2018; 12:23.doi:10.3389/fnbot.2018.00023.
-
Granier-Deferre C, et.al. A Melodic Contour Repeatedly Experienced by Human Near-Term Fetuses Elicits a Profound Cardiac Reaction One Month after Birth. PLoS one 2011; 6(2)L e17304. doi:10.1371/journal.pone.0017304.
-
Biggs MA, Gould H, and Foster DG. Understanding why women seek abortions in the US. BMC Women’s Health 2013; 13: 29.
-
Jones RK and Finer LB, Who has second-trimester abortions in the United States? Contraception 2012; 85: 544-551.
-
Foster DG and Kimport K. Who Seeks Abortions at or After 20 weeks. Perspectives on Sexual and Reproductive Health 2013; 45(4): 210-218.
-
Gianelli DM (1997, March 3). Medicine adds to debate on late-term abortion. American Medical News, 1-56
-
Rivenburg, R. (1997, April 2). Partial Truths. Los Angeles Times
-
Goldberg M. (2019, February 1). Fake News About Abortion in Virginia. New York Times.
-
Llevitan D. (2015, September 29). Clinton Off on Late-Term Abortions. Fact Check.Org. Retrieved from https://www.factcheck.org/2015/09/clinton-off-on-late-term-abortions/. On January 8, 2020.
-
Pavone, F. (2019, February 4). LISTEN: Undercover Call Catches Abortion Clinic Offering to Kill Baby at 32 Weeks. Retrieved from https://www.lifenews.com/2019/02/04/listen-undercover-call-catches-abortion-clinic-offering-to-kill-baby-at-32-weeks/. Retrieved January 8, 2020.
-
Vial, B. (2019, February 8). What It Was Like to Get a Later Abortion. Retrieved from https://www.teenvogue.com/story/what-it-was-like-to-get-a-later-abortion. Retrieved January 8, 2020.
-
Tolentino, J. (2013, September 20). Interview with Dr. Retrieved from https://www.thehairpin.com/2013/09/interview-with-dr/. Retrieved January 8, 2020.
-
Shane, M and Wilson, L. (Producers) & Shane M and Wilson, L (Directors). 2013. After Tiller (Documentary). USA. Roco Distributors.
-
Kirchoff, C. (2019, February 19). Undercover: Late Term Abortion Clinics Exposed. Retrieved from https://www.louderwithcrowder.com/undercover-late-term-abortion-clinics-exposed/. Retrieved January 8, 2020.
-
Abortions in Arizona, 2018 Abortion Report. Retrieved on June 20 from https://azdhs.gov/documents/preparedness/public-health-statistics/abortions/2018-arizona-abortion-report.pdf.
-
Barstow D. (2009, July 25). An Abortion Battle, Fought to Death. The New York Times. Retrieved from https://www.nytimes.com/2009/07/26/us/26tiller.html. January 8, 2020.
-
Boulder Abortion Clinic Abortion Services Overview. Retrieved from http://drhern.com/en/abortion-services/abortion-procedures-overview.html. Retrieved January 8, 2020.
-
Richardson JH. (2009, August 5). The Last Abortion Doctor. Esquire. Retrieved from https://www.esquire.com/news-politics/a6117/abortion-doctor-warren-hern-0909/. January 8, 2020.
-
The Editorial Board of the New York Times. (2018, December 28). Women’s Rights Part 3: The Cost of Complacency About Roe. The New York Times. Retrieved from https://www.nytimes.com/interactive/2018/12/28/opinion/pregnancy-women-pro-life-abortion.html?module=inline. January 8, 2020.
-
Hern WM. Fetal diagnostic indications for second and third trimester outpatient pregnancy termination. Prenatal Diagnosis 2014; 34: 438-444.
-
Colorado Department of Public Health and Environment, 2018 Report on Induced Terminations of Pregnancy.
-
Colorado Department of Public Health and Environment, 2019 Report on Induced Terminations of Pregnancy.
-
Guttmacher Institute. State Facts About Abortion Colorado. Retrieved from https://www.guttmacher.org/fact-sheet/state-facts-about-abortion-colorado. Retrieved on January 8, 2020
-
Goodwin TM. Medicalizing Abortion Decisions. First Things. Retrieved from https://www.firstthings.com/article/1996/03/003-medicalizing-abortion-decisions. Retrieved on January 8, 2020.
-
Hern WM. September 9, 2015. Personal Communication.
-
Carlson LM and Vora NL. Prenatal Diagnosis: Screening and Diagnostic Tools. Obstet Gynecol Clin North Am 2017; 44(2): 245-256.
-
Perinatal Hospice & Palliative Care. Retrieved from https://www.perinatalhospice.org/. Retrieved January 8, 2020.
-
Cobb AD, Acknowledged Dependence and the Virtues of Perinatal Hospice. Journal of Medicine and Philosophy 2016; 41: 25-40.
-
Wood C and Catlin A, Perinatal bereavement and palliative care offered throughout the healthcare system. Annals of Palliative Medicine 2019; 8(Suppl 1): 522-529.
-
Cunningham, FG et. al., Williams Obstetrics. McGraw Hill. 2014. Print.
-
Denny, CC. Induction of fetal demise before pregnancy termination: Practices of Family Planning Providers. Contraception 2015; 92(3): 241-245.
-
White, KO et.al., Second-trimester surgical abortion practices in the United States. Contraception 2018; 98(2): 95-99.
-
Shelmerdine SC et.al., Post-mortem Magnetic Resonance Imaging appearances of feticide in perinatal deaths. Fetal Diagn Ther 2019; 45(4): 221-229.
-
FDA. Potassium Chloride Injection. Retrieved from https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/019904s014lbl.pdf. Retrieved January 10, 2019.
-
Ovender L, Moodley J. Late termination of pregnancy by intracardiac potassium chloride injection: 5 years’ experience at a tertiary referral centre. S Afr Med J. 2012; 103(1): 47-51.
-
Society of Family Planning Clinical Guidelines. Induction of fetal demise before abortion. Contraception 2010; 81: 462-473.
-
Pincus, M. Management of digoxin toxicity. Australian Prescriber 2016; 39: 18-20.
-
Yang, EH, Shah, S and Criley, JM. Digitalis toxicity: A fading but crucial complication to recognize. The American Journal of Medicine 2012; 125(4): 337-343.
-
Moffett, BS, et.al., Serum digoxin concentrations and clinical signs and symptoms of digoxin toxicity in the pediatric population. Cardiol Young 2016; 26(3): 493-498.
-
Nucatola, D. Roth, N, and Gatter, M. A randomized pilot study of the effectiveness and side effects of two doses of digoxin as fetocide when administered intraamniotically or intrafetally prior to second-trimester surgical abortion. Contraception 2010; 81: 67-74.
-
Borgatta, L. et., al., Relationship of intraamniotic digoxin to fetal demise. Contraception 2010; 81: 328-330.
-
Finn, M. (2017, February 7). I had a Late-Term Abortion. President Trump and Pro-lifers have no Right to call me a Murderer. Slate. Retrieved from https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/019904s014lbl.pdf. Retrieved February 7, 2019.
-
Douthat, R, Goldberg, M, and Leonhardt D. (2019, February 7) The New York Times - The Argument: The Abortion Debate [Audio Podcast]. Retrieved from https://www.nytimes.com/2019/02/07/opinion/the-argument-abortion-medicare-for-all.html?emc=edit_ty_20190207&nl=opinion-today&nlid=6448792420190207&te=1. Retrieved February 7, 2019.
-
Thorp, JM. Public Health Impact of Legal Termination of Pregnancy in the US: 40 Years Later. Scientifica 2012; Article ID 980812.
-
Williams RS, Report of the Grand Jury in Re: Misc. No. 0009901-2008 County Investigating Grand Jury XXIII. Retrieved on January 8, 2020 from https://cdn.cnsnews.com/documents/Gosnell,%20Grand%20Jury%20Report.pdf.
-
Upadhyay, UD et.al., Incidence of Emergency Department Visits and Complications after abortion. Obstetrics & Gynecology 2015; 125(1): 175-183.
-
Bartlett, LA, et.al., Risk factors for legal induced abortion-related mortality in the United States. Obstet Gynecol 2004; 103(4): 729-737.
-
World Health Organization, Safe Abortion: technical and policy guidance for health systems. 2012.
-
Keyes, GR et.al., Mortality in Outpatient Surgery. Plast Reconstr Surg 2008; 122: 245-250.
-
Ahmad, J. et.al., Assessing patient safety in Canadian ambulatory surgery facilities: A national survey. Plast Surg 2014; 22(1): 34-38.
-
Media Trackers Colorado. Planned Parenthood Clinics Not Regulated by Colorado Health and Medical Standards. March 18, 2013. Retrieved from https://www.redstate.com/diary/pwatson/2013/03/18/colorado-planned-parenthood-clinics-not-regulated-by-standard-state-health-and-medical-guidelines/. Retrieved on February 16, 2019.
-
Reardon, DC and Coleman, PK. Short and long term mortality rates associated with first pregnancy outcome: Population register based study for Denmark 1980-2004. Med Sci Monit 2012; 18(9): PH71-76.
-
Pugely, AJ, et.al., Outpatient Surgery reduces Short-Term Complications in Lumbar Discectomy. Spine 2013; 38(3): 264-271.
-
Frazee, RC et.al., Outpatient Laparoscopic Appendectomy: Is it Time to End the Discussion? J Am Coll Surg 2016; 1-5.
-
Saleh, F et.al., Safety of laparoscopic and open approaches for repair of the unilateral primary inguinal hernia: an analysis of short term outcomes. The American Journal of Surgery 2014; 208: 195-201.
-
Rao, A, et.al., Safety of Outpatient Laparoscopic Cholecystectomy in the Elderly: Analysis of 15,248 Patients Using the NSQUIP Database. J Am Coll Surg 2013; 217: 1038-1043.
-
Raymond, EG and Grimes, DA. The Comparative Safety of Legal Induced Abortion and Childbirth in the United States. Obstetrics and Gynecology 2012; 119(2): 215-219.
-
Reardon, DC and Thorp, JM. Pregnancy associated death in record linkage studies relative to delivery, termination of pregnancy, and natural losses: A systematic review with a narrative synthesis and meta-analysis. Sage Open Medicine 2017; 5: 1-17.
-
Ledeerie, L et.al., Obesity as a Risk Factor for Complications after Second Trimester Abortion by Dilation and Evacuation. Obstet Gynecol 2015; 126(3): 585-592.
-
Bridges KH et.al., Maternal and procedural factors associated with estimated blood loss in second trimester surgical uterine evacuation: A restrospective cohort analysis. Int J Obstetst Anesth 2020; 6: S0959-289X(20)30032-7
-
Situ KC et.al., The duration of gestation at previous induced abortion and its impacts on subsequent births: A nationwide registry-based study. Acta Obstet Gynecol Scand 2020: 99: 651-659.
-
Steinberg JR et. al., Examining the Association of Antidepressant Prescriptions with First Abortion and First Childbirth. JAMA Psychiatry 2018; 75(8): 828-834
-
Steinberg JR et. al., The association between first abortion and first-time non-fatal suicide attempt: a longitudinal cohort study of Danish population registries. Lancet Psychiatry 2019; 6: 1031-1038.
-
Sullins DP, Abortion, substance abuse and mental health in early adulthood: Thirteen-year longitudinal evidence from the United States. SAGE Open Medicine 2016; 4: 1-11.
-
Weng S-C et. al., Do stillbirth, miscarriage, and termination of pregnancy increase risks of attempted suicide within a year? A population-based nested case-control study. BJOG 2018; 125: 983-990.
-
Luo M et. al., Association between induced abortion and suicidal ideation among unmarried female migrant workers in three metropolitan cities in China: a cross-sectional study. BMC Public Health 2018; 18: 625.
-
Wie JH et. al., The association between abortion experience and postmenopausal suicidal ideation and mental health: Results from the 5th Korean National Health and Nutrition Examination Survey (KNHANES V). Taiwan J Obstet Gynecol 2019; 58(1): 153-158.
-
Reardon, DC. The abortion and mental health controversy: A comprehensive literature review of common ground agreements, disagreements, actionable recommendations, and research opportunities. AAGE Open Medicine 2018; 6: 1-38.
-
Sullins DP, Affective and Substance Abuse Disorders following Abortion by Pregnancy Intention in the United States: A longitudinal cohort study. Medicina 2019; 55: 741.
-
Jalanko, E. et.al., Increased risk of premature death following teenage abortion and childbirth – a longitudinal study. Eur J Public Health 2017; 27(5): 845-849.